
Lessons from Rushika Fernandopulle, Former Chief Innovation Officer of One Medical and Co-founder/CEO of Iora Health, on transforming healthcare by building new models of primary care
Dr. Fernandopulle, Previous Chief Innovation Officer at One Medical, an organization dedicated to providing human-centered, technology-powered primary care to people across every stage of life.

Subscribe to our substack for weekly updates and listen on Apple Podcasts or Spotify. Connect with me if you find this post insightful and want to learn more.
Welcome back to the Pear Healthcare Playbook! Every week, we’ll be getting to know trailblazing healthcare leaders and dive into building a digital health business from 0 to 1.
Today, we're excited to get to know Dr. Rushika Fernandopulle, previous Chief Innovation Officer of One Medical, an organization dedicated to providing human-centered, technology-powered primary care to people across every stage of life.

In an acquisition that shook the healthcare industry in September 2021, One Medical completed the purchase of Iora Health - a primary care organization that prioritizes human-centered, value-based care. The deal, which amounted to a staggering $1.4 billion, was a testament to Iora Health's success in delivering high-quality care at lower costs, while improving patient satisfaction.
The visionary behind Iora is none other than Dr. Rushika Fernandopulle, who spent decades improving the quality of healthcare delivered to patients. He was the Executive Director of the Harvard Interfaculty Program for Health Systems Improvement, and Managing Director of the Clinical Initiatives Center at the Advisory Board Company. He also serves on the staff at the Massachusetts General Hospital and on the faculty of Harvard Medical School.
In this episode, Dr. Fernandopulle talks about his path to medicine, describes how he started and grew Iora Health, the acquisition by One Medical, and the future of primary care.
If you prefer listening, here’s the link to the podcast!
Changing Medicine by Studying Public Policy and Business
Dr. Fernandopulle always had a passion for serving people and found biology and medicine fascinating. After enrolling in medical school at Harvard, he realized how screwed up the healthcare system was halfway through his studies. Doctors were frustrated and patients complained about their care.
“If we created this system, then we should be able to change it for the better. I needed to learn about system change. My initial thought was to go to business school because money mattered and it was clearly driving many things in healthcare”
In the early 1990s, Rushika approached folks at Harvard medical school with the idea of studying business, but he met some resistance. He was told that if he went into business school, he may not be welcomed back into medicine.
I remember them saying “Look son, you could be one of us (medicine) or one of them (business). If you go over to the business side, it’s not just bad, it’s evil and it’s the dark side.
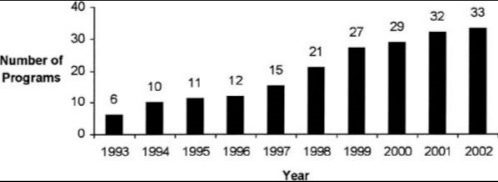
In 1993, only 6 medical schools offered the joint MD/MBA program. It wasn’t common back then, but the dual-degree program has been steadily rising. Now in 2023, 82 programs offer the MD/MBA.

Instead of pursuing a business degree, Rushika decided to go to the Kennedy School for Public Policy, which was more acceptable in the eyes of the medical administration. So while pursuing his Master’s in Public Policy, he also took some classes in the business school with the goal of thinking about systems change in medicine.
“Years later, I was fortunate to run the Harvard Interfaculty Program for Health Systems Improvement. Harvey Fineberg, was provost at Harvard at the time. And he had this insight that Harvard ought to try and lend its intellectual weight to solving great problems like healthcare. We realized fixing healthcare isn’t a medicine, business, public health, public policy, or economics problem. We needed to be able to cut across these silos. The goal of the Faculty Program was to draw from all the different schools and cut across these silos to solve healthcare from an interdisciplinary point of view.”
Why an Incremental Change Model Does Not Always Work
While leading the interfaculty program, Rushika also practiced as a primary care physician on the side. There were many nights that he had a full day of patients. He would not have time to go to the bathroom, eat lunch, and even had to skip dinner with his family as he was finishing up notes.
“I’d sit there for hours writing my notes and making sure I didn’t get yelled at for not meeting our RVUs. I had a colleague tell me everyday, I lose a little piece of my soul. Patients come to us with such big needs. And we have all this training, but the system doesn't allow us to help them.”
Rushika couldn’t see himself spending the next 30 years of his career beating his head against the wall in a terrible system. He tried working within the system to fix it. He sat on committees, did advisory boards, and worked on policy in Washington.
“There is the belief in an incremental change model, which is taking an existing practice or hospital and tweaking it bit by bit. Yet, that does not work in a system that is rotten to its core. Healthcare in this country was built around a series of transactions, and the last I checked, transactions don’t heal people. A new model needed to be built based on relationships.”
Instead of going through an incremental change model and innovating from the top-down, Dr. Fernadopulle wanted to go bottom-up and start with the healthcare consumer.
“I went to all the big health systems in town in Boston and asked them to let me build a new model of primary care focused on relationships in just one of their practices. They had thousands of practices and all I wanted was just one. They all sort of patted me on the head and said, “That’s really interesting but our practices are full, we are making money, what’s the problem?
Undeterred by the reluctance of big health systems in Boston to let him build a new model of primary care, Rushika made a bold move. He quit his job and embarked on a mission to rebuild the primary care system from scratch, based on relationships.
How It Started with Iora Health
Most people would think quitting a stable job as a doctor to start a new model of care in a practice would be risky. Rushika believes that if there is anyone in the world who should not be risk averse, it is a doctor.
If your entrepreneur endeavor does not work out as a doctor, you can get a job anywhere. You can pick up the phone and get a job as a clinical doctor in about 10 minutes. You can moonlight, work in nursing homes, and so many other things. Just don’t be afraid to take risks because the worst thing that happens is that it doesn't work out and you learn something! Risk is overrated particularly for people who are doctors.
In April of 2004, Rushika took a leap of faith and opened a practice called Renaissance Health, the rebirth of primary care. It started with 1 little practice in Arlington. No one at the time cared about primary care and so the entire venture was initially funded by good old-fashioned bootstrapping.
“We went to Home Depot and painted the practice ourselves. We drove to the closest IKEA, and hired a bunch of BU guys for some pizza and beer to help us put things together.”
The vision of care that the team had was radically consumer-centric, value-based, digital, and was ahead of its time. The model gave people health coaches, integrated behavioral health needs, emailed and texted patients to maintain transparency, and even gave patients access to their medical records to empower them in their care. But this model was not without its challenges as insurance companies were hesitant to reimburse these additional services.
“In 2004, no one did this because the fundamental problem is that insurance companies will never pay for all of this. When I took my Hippocratic Oath, I said I would serve my patients and not the insurance company.”
The early primary care practice asked each patient to pay about $40/month to help them break even. If patients had more money, they could pay more or if they were poor they could pay less. Everyone just had to pay something to get the care they needed.
Theory of Change Rooted in the Consumer and Patient Experience in Healthcare
The team at Iora was not trying to directly change an existing medical group or practice. Their theory of change was rooted in providing a better patient and consumer experience than the existing health systems and practices.
Under the fee-for-service model patients are seen for less than 30 minutes, tests are ordered, medications are prescribed, and the patient is ultimately left on their own until they see the provider months later.
At Iora Health, they wanted to continue to be with the patient beyond the clinical visit. The health coach and other staff members would continuously be in contact with the patient to accompany them in their medical journey.
“We had a new vision of taking care of our patients. If existing health systems didn't like it, I would tell them to keep doing what they’re doing, but I would mumble under my breath, someday we would take their patients.”
Patients were voting with their feet and Iora Health grew from 1 practice in 2004 to over 48 practices by 2020. Their program reduced hospitalizations by 40%, cut ER visits in half, and reduced total healthcare costs by 20%. A Harvard Business Review article highlights these statistics and more.
Disrupting the Status Quo Through Purposeful Partnerships
The Iora Health team believed that they were providing a superior patient experience and reducing overall costs by emphasizing primary care and preventing hospitalization, but they faced challenges in obtaining medical data from payers. Additionally, some accused Iora of raising expectations and making other medical practices in Boston appear inadequate.
Rushika acknowledged that disrupting the status quo was their goal. However, Harvard Pilgrim, a major health plan, expelled Iora from their network, hindering their growth. To overcome this obstacle, the team realized they needed to pivot to a new approach and form a partnership with an organization that would benefit from lower healthcare costs. This insight spurred the idea to go to big employers to create a purposeful partnership.
“We teamed up with a guy named Arnold Milstein, a doctor who worked for Mercer Health and Benefits. He got us a partnership with the Boeing company. Just like what we did in Arlington, we were asked to do the same thing in Seattle for Boeing employees by working with some of these big health systems that Boeing used like Virginia Mason, Everett Clinic, and Valley Medical Center.”
By working with Boeing, Iora Health was able to leverage this huge employer to be able to get their medical data from payers. If Boeing ever requested or asked for the healthcare data, they would get it right away compared to Iora Health requesting prayers for the data on their own. In addition to Boeing, Iora Health also worked with the casino workers in Atlantic City. These purposeful partnerships involved employers paying the fee for Iora Health and helping the team collect data that delineated the incredible results of reducing hospitalizations, ER visits, and cutting down total spending.
Through these purposeful partnerships, Iora Health delivered significant benefits to the employers by reducing healthcare costs and creating alignment among all stakeholders. By enhancing health benefits and decreasing costs, Boeing could better compete against their primary competitor, Airbus, and the casino workers' employers avoided strikes related to healthcare expenses.
Raising Money as One of the Earliest Tech-Enabled Healthcare Service Organizations
In 2011, Atul Gawande wrote an incredible piece in the New Yorker entitled “The Hot Spotters.” The article featured Rushika’s model of care in Atlantic City and how effective it was in cutting costs while providing high-quality care. The article led to a flood of phone calls for Rushika as more people became aware of his work. He decided at that point it was finally time to raise capital and scale his model.
“It’s great to do these little pilot projects but that is not going to change the world. What we need to do is scale our intervention and frighten people in healthcare that we're going to take their patients away or they better start doing what we're doing.
In 2011, Iora Health raised its first capital as one of the first primary care and tech-enabled healthcare practices. During that time, it was rare for investors to invest in primary care. It was heavily underfunded, underutilized, and the return on investment would take time. Primary care cannot be improved in just a couple of months or years because it takes time and the Iora team was purposefully looking for investors who understood that.
“My co-founder at the time was Chris McKown, who previously co-founded and sold Health Dialog and made a bunch of money. It was easier for us to raise money by having a previous founder. So we've got three local Boston Area VC firms who believed in our mission and had a long-term view for their investment. They stuck with us for 11 years until they ever got any sort of exit.
In Iora’s second investment round, Tony Hsieh, the CEO of Zappos, led the investment.
“When Tony expressed interest in meeting with me, I flew out to Las Vegas to chat with him. We met up at a downtown cocktail lounge at 11:30 pm, where I had to use a secret knock to get in (which was apparently Tony's style). During our conversation, Tony mentioned that he was working on a downtown project in Las Vegas and needed someone to build a healthcare practice for his employees. I offered to take on the project, and he asked about our fundraising. I told him that we were raising a $10 million round, and when he inquired about the company's valuation, I gave him a number on the spot: $28 million. To my surprise, Tony agreed and asked where he could send the check."
No pitch deck was used and no business model was talked about between Rushika and Tony. Tony loved the idea and liked Rushika and that was all the conviction he needed to lead the round. Investors don't just invest in a business plan or strategy, they invest in the people behind it. A compelling idea may pique their interest, but it's the founders' passion, vision, and ability to execute that truly captures an investment.
Acquisitions that Can Transform Healthcare
The motive behind starting Iora Health was to transform healthcare. After 6 rounds of venture money, lots of companies started approaching the team, especially different health plans. Rushika thought to himself that what the world really needed was strong, independent primary care.
“I thought about what I wanted for myself and my family. It was really simple. I wanted a primary care doctor that works for us and not the health system. I didn’t want to feed the beast and sell it to a health plan. I didn’t view One Medical, Oak Street, ChenMed, and others as my competitors. If you add all of us up we are just a rounding error in the entire healthcare ecosystem. To enact change in healthcare we needed to put all these value-based care organizations together.”
Rushika frequently engaged in conversations with Amir Rubin, CEO of One Medical, regarding combining the two organizations together. One Medical was in the retail space and had a membership model that evolved into serving employers, but they never jumped into Medicare. Iora Health made the endeavor to engage with full risk Medicare patients. The combination of these two organizations would help provide continuous and comprehensive care for inter-generational population health, across adjacent commercial and Medicare markets.
“There is this misguided view that the whole job of a company is to optimize shareholder return. But that is flawed. You need to serve your customers, your employees, the broader community, and then bring value to your shareholders. There needs to be alignment among all four of these stakeholders. For us, merging with One Medical continued that alignment and helped us scale our mission.
When founders are thinking about Mergers and Acquisitions, they need to remember the importance of alignment between the mission of the organizations. They also need to consider culture. Many of the reasons that an acquisition doesn’t go well is due to a cultural mismatch.
“I knew Tom Lee who started One Medical for years. Both Iora Health and One Medical evolved together. Some of our doctors and workers went to One Medical to learn and vice versa. Both organizations wanted to change healthcare and both were tech-savvy. Our models weren’t quite the same, but there was a cultural fit between the organizations and that is what made the integration between One Medical and Iora seamless.”
What Makes Innovating in the Medicaid Space Difficult
Both One Medical and Iora had a strong interest in the Medicaid space as both organizations were bent on transforming healthcare for everyone and Medicaid covers approximately 20% of the US population. It was easy for Iora to provide care to dual-eligible patients (those with Medicare and Medicaid). But serving individuals just with Medicaid was a struggle. There are at least 3 challenges with serving Medicaid.
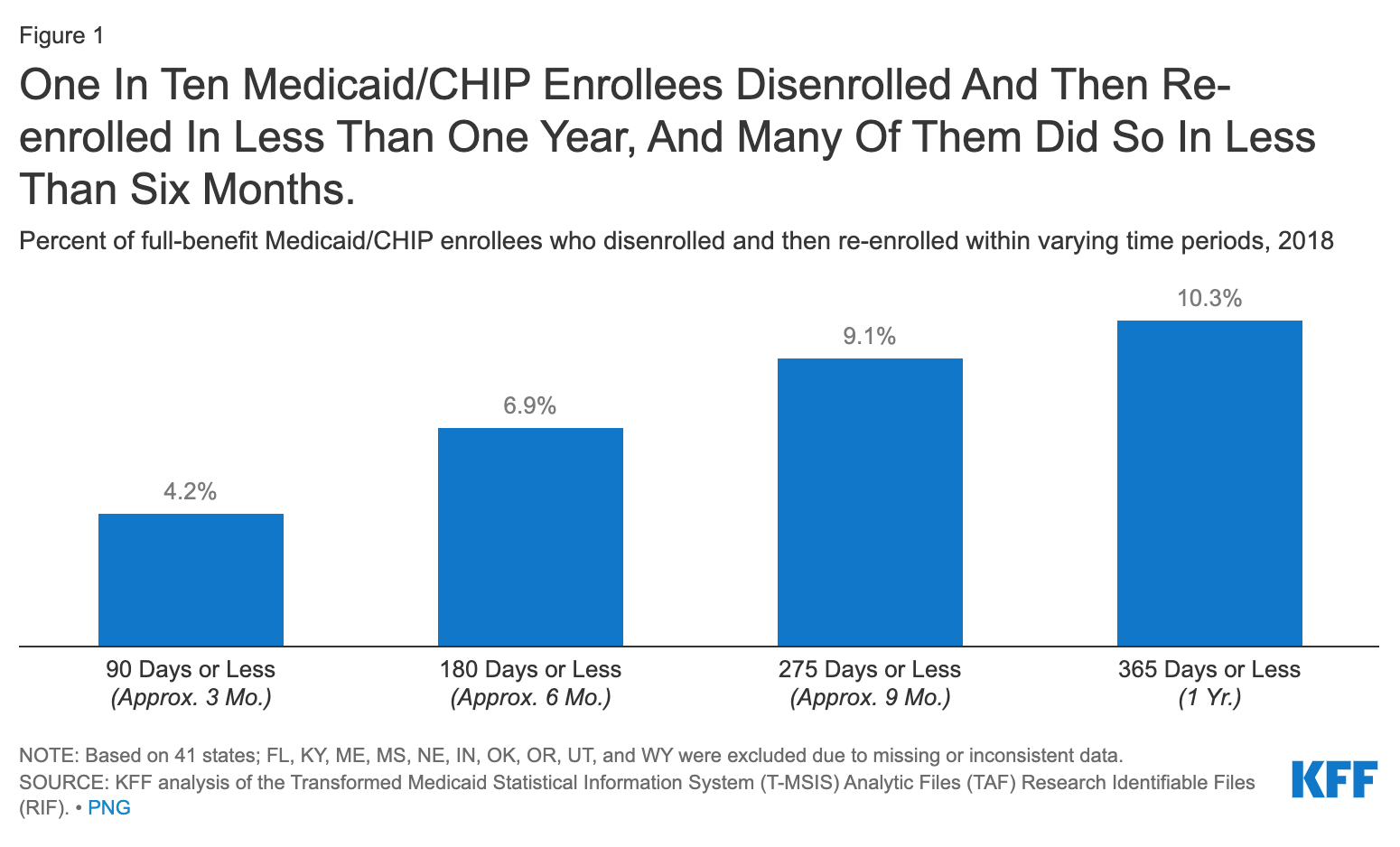
Churn Rate (biggest reason)
In most state Medicaid programs there is an incredible churn rate. Churn occurs when there is a temporary loss of Medicaid coverage in which enrollees disenroll and then re-enroll within a short period of time. This can be due to enrollees experiencing short-term changes in income or circumstances (work hours) that make them temporarily ineligible.
For primary care to work effectively, you have to change people’s behavior and work with them over a continuous period of time for years. A high churn rate prevents that from happening.
Qliance, one of the first direct primary care (DPC) practices in Seattle, took a managed medicaid contract from Centene to serve 15,000 medicaid patients. They had a 80% churn rate from years 1 and 2 and Qliance eventually went out of business.
States need to zero out their Medicaid budget
States need to zero out their Medicaid budget every year, which makes it difficult to figure out a way to invest in one year to see a return in the next. This lack of investment hinders the ability to implement effective longitudinal care models.
There is the complex regulatory and advocacy landscape
The varying regulations from state to state and a belief that fee-for-service is the only payment model that works for Medicaid add to the challenge.
Despite these obstacles, One Medical is forging ahead with a pilot program for Medicaid in DC.
“Medicaid has to fix itself. It needs to stop the churn and these other problems because it becomes an unwinnable game. We need to implement longitudinal care models and move away from the idea that fee-for-service is the only payment model that works for Medicaid.”
Advice to Founders on Building Successful Healthcare Companies
There are huge opportunities to innovate in healthcare.
Healthcare offers huge opportunities for innovation, with the potential to transform patient outcomes and generate significant economic returns. The healthcare industry is ripe for disruption, with a multitude of problems waiting to be solved by innovative entrepreneurs like you. Whether it's improving patient access to care, reducing healthcare costs, or enhancing the quality of care provided, there is no shortage of problems to tackle.
It takes time
Building a successful healthcare company is a long-term endeavor, and quick profits should not be your primary goal. The healthcare industry is complex and heavily regulated, which means that it can take years of hard work to gain traction and make a real impact. For example, Iora Health started 20 years ago and it took many years to achieve a successful exit. So, if you're looking to make money quickly, healthcare might not be the right place for you.
Always think about alignment between your stakeholders
To achieve success in healthcare, it is essential to prioritize alignment between stakeholders. This means aligning your company culture, hiring the right people, partnering with investors who share your vision, and collaborating with other companies that can help you achieve your goals.
Don’t take shortcuts
It is crucial to avoid taking shortcuts when it comes to healthcare. While the idea of moving fast and breaking things may have worked for some technology companies, it doesn't translate well to healthcare. Companies in the healthcare industry are dealing with people's health and well-being, which means that there is little room for error. It is essential to prioritize patient safety and well-being above all else, and to take a more deliberate and cautious approach to innovation in healthcare.
Thanks for reading Pear Healthcare Playbook! Subscribe for free to receive new posts and support my work.
Interested in One Medical or joining their team? Learn more on their website, Twitter, and LinkedIn.
A note from our sponsor: PacWest
Looking for guidance, connections, resources, opportunity? Pacific Western Bank’s banking products and services are built to support your evolving needs as you navigate the challenges of growing a successful business. As you continue to scale, our team will be with you every step of the way. Ready to take your business to the next level? Learn more: pacwest.com